Carpal tunnel syndrome (CTS) is the name of a group of problems that includes swelling, pain, tingling, and loss of strength in your wrist and hand. Women are three times more likely to have carpal tunnel syndrome CTS than men.
Carpal Tunnel Syndrome (CTS) in women is a common condition caused by compression of the median nerve as it passes through the carpal tunnel in the wrist. Women are more frequently affected than men, possibly due to hormonal fluctuations that can cause fluid retention and increased intracarpal pressure. Anatomical factors, such as a naturally smaller carpal tunnel, also predispose women to CTS. Pregnancy, menopause, and conditions like hypothyroidism and diabetes further increase risk by contributing to swelling and nerve inflammation. The compression leads to symptoms such as numbness, tingling, and weakness in the hand and fingers, particularly affecting the thumb, index, and middle fingers. Nighttime symptoms are prominent due to wrist flexion during sleep. Diagnosis typically involves a clinical examination, nerve conduction studies, and electrophysiological tests to assess median nerve function.
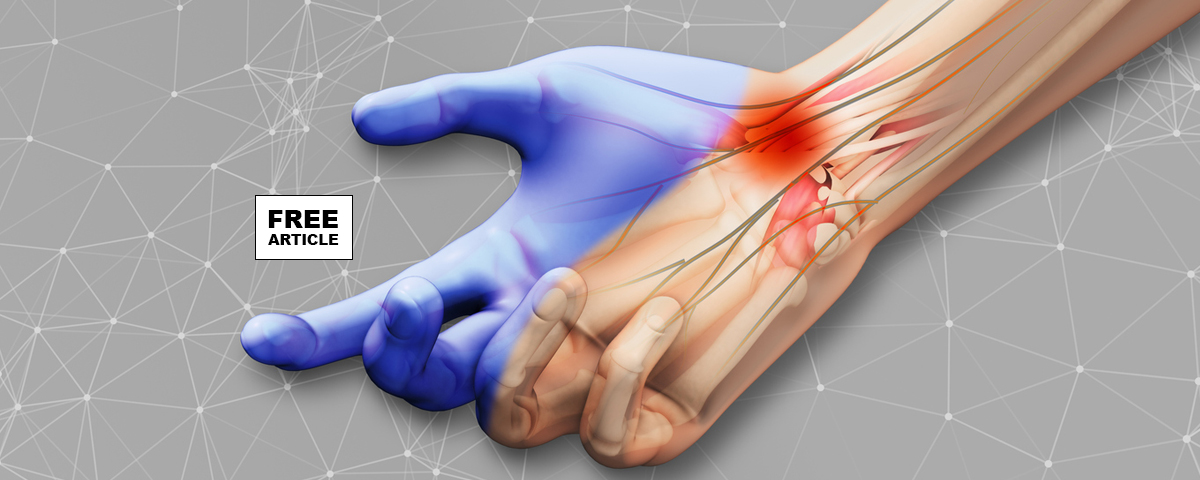
Understanding the mechanism underlying carpal tunnel syndrome also allows us to understand why certain actions and risk factors may lead to the development of, or even episodic worsening of, the syndrome. Common signs associated with carpal tunnel include aggravation of symptoms at night, while driving, on the phone, or typing on a computer keyboard. As one may have guessed, most of these scenarios (and similar ones that are CTS-associated) involve the individual flexing their wrists, which further compresses the carpal tunnel onto itself leading to an increase in pressure to the area. Another common sign of CTS is paresthesias, numbness or tingling, in the thumb, index, middle, and medial half, the inner side, of the ring finger on the palm of the hand. These finding can also be explained by an understanding of the anatomy. After the median nerve crosses the carpal tunnel in the hand, it supplies the sensory innervation to these digits. Naturally, compression of the nerve explains the burning/tingling sensation in the sensory distribution of the nerve that many afflicted individuals complain of.
The size of the carpal tunnel varies between men and women, with women generally having a smaller carpal tunnel compared to men. This anatomical difference contributes to the higher prevalence of Carpal Tunnel Syndrome (CTS) observed in women, as the reduced space makes the median nerve more susceptible to compression from swelling, repetitive movements, or fluid retention. Studies have shown that the median nerve and the dimensions of the carpal tunnel are smaller in women, particularly in those with a naturally narrower tunnel. This anatomical predisposition, combined with hormonal influences and other risk factors, explains why women are more frequently affected by CTS than men.
Hormonal fluctuations related to pregnancy, menopause, and conditions like hypothyroidism can lead to fluid retention and swelling in the wrists, exacerbating nerve pressure. Women are also more likely to engage in repetitive hand activities, such as typing, which increase the risk of developing CTS due to repeated strain. Medical conditions prevalent in women, including rheumatoid arthritis and diabetes, contribute to systemic inflammation and potential nerve damage, further heightening vulnerability. Obesity also plays a role by increasing fatty deposits that may compress the median nerve. Genetics can influence susceptibility, as a family history of CTS increases risk. Additionally, lifestyle factors like smoking can impair blood circulation and nerve health. Addressing these risk factors through ergonomic interventions, managing chronic health conditions, and adopting a healthy lifestyle can be crucial in preventing or mitigating CTS in women.
Treatment for CTS in women focuses on relieving pressure on the median nerve. Initial management includes lifestyle modifications, such as wrist splinting, especially at night, to maintain a neutral wrist position and reduce nerve compression. Nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroid injections may offer temporary symptom relief by reducing inflammation. If conservative measures are ineffective, surgical intervention, such as carpal tunnel release, may be necessary, which involves cutting the transverse carpal ligament to relieve pressure on the median nerve. Early diagnosis and treatment are crucial in preventing permanent nerve damage and restoring normal hand function. Women’s specific health factors, such as hormonal changes, should be considered when managing and preventing CTS to ensure effective treatment outcomes.