Psoriasis is a chronic, autoimmune skin condition characterized by the overproduction of skin cells, leading to the formation of raised, red, scaly plaques on the skin. These plaques can appear anywhere on the body, but are commonly found on the elbows, knees, scalp, and trunk. Psoriasis is not contagious and is caused by an overactive immune system that mistakenly attacks healthy skin cells.
Psoriasis presents as several distinct clinical types, each characterized by unique lesion morphology, affected body regions, and varying responses to treatment. As the most prevalent form of psoriasis, plaque psoriasis is characterized by round or flat, erythematous plaques with a distinctive pink base covered by silvery-white scales. These plaques commonly occur on areas such as the elbows, knees, scalp, and lower back. The condition is often accompanied by varying degrees of pruritus, itchiness, which can range from mild to severe, significantly affecting patient comfort and quality of life.
Additional types of psoriasis comprise about 10% of cases. These include Guttate, Pustular, and Erythrodermic.
Guttate psoriasis is identified by small, discrete red papules, typically ranging from 1 to 10 millimeters in diameter, with minimal scaling. Guttate psoriasis often appears suddenly, often triggered by a streptococcal infection, such as strep throat.
Pustular psoriasis is further divided into generalized pustular psoriasis (GPP), localized forms such as palmoplantar pustulosis (PPP) and acrodermatitis continua of Hallopeau (ACH). Generalized pustular psoriasis GPP is marked by a rapid eruption of sterile pustules on a background of red, inflamed skin, often accompanied by systemic symptoms like fever, fatigue, and muscle weakness, which can necessitate urgent medical attention due to potential complications. Palmoplantar pustulosis PPP manifests as sterile pustules on the palms and soles, associated with erythema, scaling, and thickening of the skin (keratoderma). Acrodermatitis continua Hallopeau ACH is a condition characterized by recurrent pustules on the tips of the fingers. Patients may experience osteolysis, the destruction or dissolving of bone tissue which has a significant impact on quality of life.
Erythrodermic psoriasis is a rare but severe form of psoriasis, characterized by extensive erythema and exfoliation covering more than 75% of the body’s surface area. Erythrodermic psoriasis often arises as an exacerbation of another psoriasis subtype or in response to triggers such as infection, withdrawal of systemic psoriasis treatment, or stress. Due to its widespread inflammation, this form can lead to systemic complications, including fluid and electrolyte imbalances, thermoregulation disturbances, and increased risk of infection.
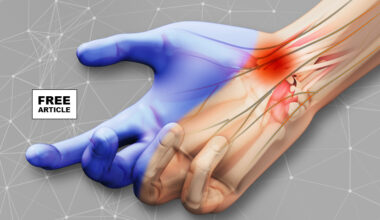
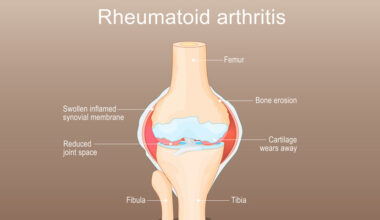
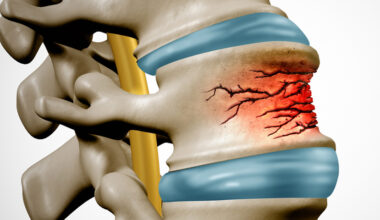
Psoriatic arthritis (PsA) is a chronic inflammatory arthritis associated with psoriasis. PsA commonly involves the small joints of the hands and feet, but larger joints such as the hips, knees, and spine may also be affected. Symptoms include joint pain, swelling, and stiffness, which can be disabling and may occur either in conjunction with or independently of skin lesions.
Psoriasis can affect the nails and produces a variety of changes in the appearance of fingers and toenails. Nail psoriasis occurs in 40–45% of people with psoriasis affecting the skin, and has a lifetime incidence of 80–90% in those with psoriatic arthritis. These changes include pitting of the nails (pinhead-sized depressions in the nail is seen in 70% with nail psoriasis), whitening of the nail, small areas of bleeding from the capillaries under the nail, yellow-reddish discoloration of the nails known as the oil drop or salmon spots, dryness, thickening of the skin under the nail (subungual hyperkeratosis), loosening and separation of the nail (onycholysis) and crumbling of the nail.
Psoriasis has multifactorial causes, with a significant genetic predisposition contributing to disease risk. To date, over 60 susceptibility loci have been identified, with the HLA-Cw6 allele, one of the two versions of the gene that is inherited from each parent, being particularly associated with early-onset psoriasis. Environmental factors, including psychological stress, physical trauma (known as the Köbner phenomenon), and lifestyle choices, such as smoking, further influence disease expression. Notably, while smoking is known to increase the risk of developing psoriasis in the general population, recent studies indicate that it may, paradoxically, reduce the likelihood of developing psoriatic arthritis among those affected by psoriasis.
The pathogenesis of psoriasis is intricately linked to T cell immunity. The disease process begins with the activation of antigen-presenting cells (APCs) within the skin, such as dermal dendritic cells and epidermal Langerhans cells, in response to external or internal antigens, including skin trauma or infection. Upon activation, these antigen-presenting cells APCs migrate from the skin to nearby lymph nodes, where they present antigens to naive CD45RA+ T cells, ultimately initiating T cell activation in keratinocyte cells, the outermost layer of skin, the epidermis. T cells migrate into these affected skin cells and release cytokines that drive keratinocyte hyperproliferation, disrupt normal cellular differentiation, and perpetuate inflammatory responses through positive feedback loops in cell signaling. This cascade results in the sustained formation of psoriatic skin lesions. Therefore, cell signaling pathways are central to the pathogenesis of psoriasis. Understanding these pathways is crucial for developing effective therapeutic approaches, as they represent key intervention points in managing the disease.
The diagnosis of psoriasis is usually based on the appearance of the skin. Skin characteristics typical for psoriasis are scaly, erythematous plaques, papules, or patches of skin that may be painful and itch. No special blood tests or diagnostic procedures are usually required to make the diagnosis.
The differential diagnosis of psoriasis may be crucial and includes eliminating dermatological conditions similar in appearance such as discoid eczema, seborrheic eczema, pityriasis rosea that may be confused with guttate psoriasis; nail fungus which may be confused with nail psoriasis and even cutaneous T cell lymphoma since 50% of individuals with this cancer are initially misdiagnosed with psoriasis. Dermatologic manifestations of systemic illnesses such as the rash of secondary syphilis may also be confused with psoriasis.
If the clinical diagnosis is uncertain, a skin biopsy or scraping may be performed to rule out other disorders and to confirm the diagnosis. Skin from a biopsy shows clubbed epidermal projections that interdigitate with the dermis on microscopy. Epidermal thickening is another characteristic histologic finding of psoriasis lesions. The stratum granulosun layer of the epidermis is often missing or significantly decreased in psoriatic lesions; the skin cells from the most superficial layer of the skin are also abnormal as they never fully mature. Unlike their mature counterparts, these superficial cells keep their nuclei. Inflammatory infiltrates can typically be seen on microscopy when examining skin tissue or joint tissue affected by psoriasis. Epidermal skin tissue affected by psoriatic inflammation often has many CD8+ T cells, while a predominance of CD4+ T cells makes up the inflammatory infiltrates of the dermal layer of skin and joint.
Psoriasis is not just a skin disease. The symptoms of psoriasis can sometimes go beyond the skin and can hurt the quality of life of the affected individuals. Additionally, the co-morbidities increase the treatment and financial burden of psoriasis and should be considered when managing this condition.
Cardiovascular Complications
There is a 2.2 times increased risk of cardiovascular complications in people with psoriasis. Also, people with psoriasis are more susceptible to myocardial infarction (heart attack) and stroke. It has been speculated that there is systemic inflammation in psoriasis, which drives “psoriatic march” and can cause other inflammatory complications including cardiovascular complication. A study used fluorodeoxyglucose F-18 positron emission tomography-computed tomography (FDG PET/CT) to measure aortic vascular inflammation in psoriasis patients, and found increased coronary artery disease indices, including total plaque burden, luminal stenosis, and high-risk plaques in people with psoriasis. Similarly, it was found that there is an 11% reduction in aortic vascular inflammation when there is a 75% reduction in the Psoriasis Area and Severity index (PASI) score.
Depression
Depression or depressive symptoms are present in 28–55% of people with psoriasis. People with psoriasis are often stigmatized due to visible disfigurement of the skin. Social stigmatization is a risk factor for depression; however, other immune system factors may also be related to the observed increased incidence of depression in people with psoriasis. There is some evidence that increased inflammatory signals in the body could also contribute to depression in people with chronic inflammatory diseases, including psoriasis.
Type 2 Diabetes
People with psoriasis are at approximately 50% increased risk of developing type 2 diabetes A genome -wide genetic study found that psoriasis and type 2 diabetes share four loci, namely, ACTR2, ERLIN1, TRMT112, and BECN1, which are connected via the inflammatory NF-κB pathway.